
Articles, videos about Tongkat Ali, Black Ginger, and Butea Superba
Articles, videos about optimal sex
A skeptical patient
There is no denying of the extraordinary blessings, Western medicine has brought to mankind; anatomy, anesthesia, and antibiotics: vaccines and Viagra.
There is also no denying that lotteries and gambling have made some winners very rich.
The largest ever lottery win by a single person was 877.8 million US dollars on October 23, 2018, in South Carolina. Taker unknown.
French Roulette is supposed to have the highest RTP (return to player) ratio, between 98 and 99 percent. But everybody knows that casinos have a history of mafia-style cheating. Rational people don't gamble. Prominent example: Howard Hughes, then one of the richest men in the world, rented the top 2 floors of the Las Vegas Desert Inn as his residence, but then angered the mob-affiliated operators who expected him to be a high-roller by not gambling at all.
But while gambling is irrational just because of an on-average miserable ROI (return on investment), private health insurance catapults you into the fangs of a healthcare system where more emotional risks lurk.
The science of anatomy started with the vivisection (dissection of living bodies) performed on humans by Herophilos of Alexandria (335BC-280BC). But while one may see more by dissecting a living body (for example a pumping heart), human vivisection was probably rare, even in ancient history.
A dissection of a dead body is shown in a famous piece of art (see below), painted by Rembrandt in 1632.
In medieval times, the vivisection of humans was not done because the Church and ordinary people were against it... not necessarily out of empathy towards murderers. Rather, the Church was afraid of released souls, the dominion of God; and ordinary people feared that the dissection of living or dead human bodies would set free a whole assortment of ghosts and zombies.
Frogs never were, and still aren't, so fortunate. While anatomical studies on living higher animals such as cats, dogs, and monkeys are ferociously opposed by animal rights activists, the dissection or vivisection of frogs is standard fare at medical schools and faculties of life sciences, and part of the curriculum of high schools. Sometimes, amphibian dissection is performed for elementary pupils. The footage below shows Asian girls utilizing a sewing kit to perform a vivisection on a frog. Take notice of the throbbing heart of the poor creature towards the end of the clip.
While upcoming surgeons practice a lot on animals, they sooner or later must get their hands on living human patients to practice their skills; the same goes for medical students and interns in hospitals. This probably leads to overtreatment for the purpose of gaining experience, apart from providing an opportunity to bill for a procedure, especially when an insurance, rather than the patient, pays for it.
"Two decades later, after witnessing similar pre-death rituals countless times, Meier published the story of a 73-year-old man with metastatic lung cancer who told his doctors he didn’t want invasive testing and treatment. His doctors consulted a psychiatrist, who said the man was "in denial" about his illness. After some pressure from his doctors, the man and his family agreed to further diagnostic testing and treatment, including placement of a gastrostomy tube. He was ultimately subjected to 47 days of painful and invasive treatments before dying."
[Source: Unnecessary care - Is profit driven healthcare to blame?]
"At 87, Maxine Stanich cared more about improving the quality of her life than prolonging it. She suffered from a long list of health problems, including heart failure and chronic lung disease that could leave her gasping for breath. When her time came, she wanted to die a natural death, Stanich told her daughter, and signed a "do not resuscitate" directive, or DNR, ordering doctors not to revive her should her heart stop. Yet a trip to a San Francisco emergency room for shortness of breath in 2008 led Stanich to get a defibrillator implanted in her chest — a medical device to keep her alive by delivering a powerful shock. At the time, Stanich didn't fully grasp what she had agreed to, even though she signed a document granting permission for the procedure, said her daughter, Susan Giaquinto.
"That clarity came only during a subsequent visit to a different hospital, when a surprised ER doctor saw a defibrillator protruding from the DNR patient's thin chest. To Stanich's horror, the ER doctor explained that the device would not allow her to slip away painlessly and that the jolt would be 'so strong that it will knock her across the room,' said Giaquinto, who accompanied her mother on both hospital trips. Surgery like this has become all too common among those near the end of life, experts say....
"The practice is driven by financial incentives that reward doctors for doing procedures... The cost of these surgeries — typically paid for by Medicare, the government health insurance program for people over 65 — involve more than money... Older patients who undergo surgery within a year of death spent 50 percent more time in the hospital than others, and nearly twice as many days in intensive care... More than 12 percent of defibrillators were implanted in people older than 80, according to a 2015 study... The total cost of the procedure runs about $60,000... Surgery poses serious risks for older people, who weather anesthesia poorly."
[Source: Surgery Near End of Life Is Common, Costly
What does "older people, who weather anesthesia poorly" mean exactly? Anesthesiologists are afraid to dose generously in the elderly, as an overdose could lead to death, and a malpractice lawsuit. But if they underdose, there is a real risk of anesthesia awareness... being mentally awake during surgery and feeling all the pain while at the same time not being able to move at all because of an effective muscle relaxant. Then your experience is comparable with that of the frog in the video above.
How often does anesthesia awareness happen? A recent figure puts the risk in between 1 in 100 and 1 in 1000. [Source: Awareness during anesthesia: a problem without solutions?]
Another risk of major surgery in the elderly is postoperative delirium which affects 10 to 70 percent of surgery patients over 60. [Source: Anesthesia awareness. Can midazolam attenuate or prevent memory consolidation on intraoperative awakening during general anesthesia without increasing the risk of postoperative delirium?]
I have a vital interest in that in advanced age, no money can be made by rolling me through a healthcare system, neither for-profit, nor for fame, nor for practice, and not even for scientific knowledge. To have no health insurance is a good start.
In the early years of the third millennium, I wrote an ideology based on two parameters. The ideology (several hundred pages) can be summarized as: A comfortable death, and, before that, optimal sex. That is what life is about. Mind you: it is not formulated as optimal sex and then a comfortable death. A comfortable death is the primary concern.
Dying can be such a horror that when you quantify by value all the good things you experienced in life and set this off against the quantified-by-value agony of death, you may end up with a negative balance. If that is the case, suicide is a rationally preferable option.
When I am old and in a coma, or even just unconscious after an accident that will kill me if I am left alone, then I do NOT want to be resuscitated. I just want to be dead. Death will anyway soon arrive. So I will be thankful to be through, without more suffering.
Not being health-insured at least eliminates some for-profit forms of unwanted medical intervention. Living at a remote location can be another precaution.
Sure, I am in favor of some procedures of modern Western medicine. I opt for local anesthesia when I need a tooth extracted, The Western science of anesthesia, incidentally, was started by two American dentists, Horace Wells (1815-1848) and William Morton (1819-1868). I am in favor of most vaccinations, including Pfizer-BioNtech's Covid-19 shots. I use medications like antibiotics, even Viagra.
But the argument that I may need really expensive medications in case I develop a strange disease won't sell me an insurance policy.
Apart from trying to prevent harm to my health in the first place, rather than trying to ameliorate harm after it has been done, I am convinced that gentle herbal approaches to ailments are undervalued by modern Western medical science. Herbal remedies, of course, don't fit easily into the business model of big pharma and the physician-centered healthcare apparatus. Herbals can't be patented to protect against competition to exorbitant prices, and when they don't require prescriptions, they deprive physicians of the authority they so enjoy.
In contrast to, for example, Traditional Chinese Medicine, TCM, or Ayurvedic practices, gentle herbal approaches to healing are not a big part of the modern Western Materia Medica. This in spite of Hippocrates (460BC-370BC), whose oath (primum non nocere - First do no harm) physicians have to swear before being admitted to the board. Hippocrates proclaimed "Let food be thy medicine". If you are curious, try searches on scholar.google.com for "turmeric inflammation" or "ginger rheumatism" or, for that matter, "tongkat ali rho kinase". Mind you, too, that tea (Camellia sinensis) as an antidote to fatigue comes from Asian herbal medicine, and so do opium and cannabis.
One difference between herbals and Western pharmaceutical drugs is that herbals have a shared evolutionary history with other forms of life, including humans, while most modern pharmaceuticals are xenobiotics. And while some xenobiotics can be used to ameliorate certain conditions, the chances are 99.999 percent that xenobiotics have long-term detrimental effects.
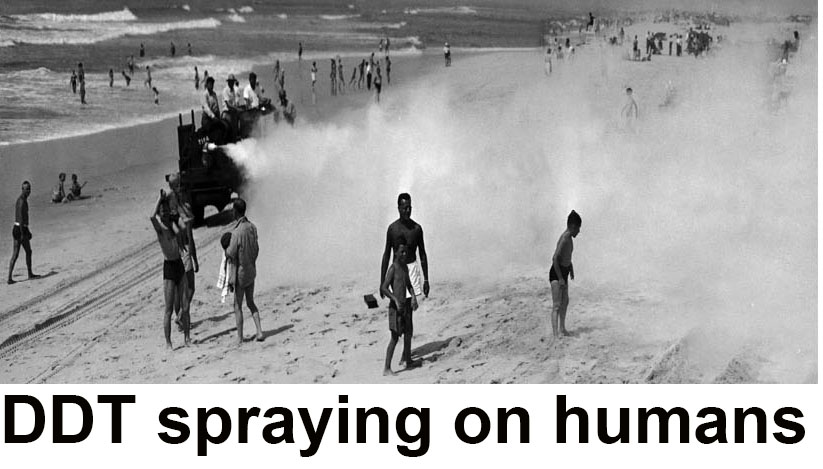
The underestimation of long-term adverse effects of synthetic chemicals is a common occurrence in the chemical-pharmaceutical industry. The insecticide DDT, too, was initially considered harmless to humans.
The American surgeon most notorious for using lobotomy to engineer humans with reduced impulses and limited or no free will was, ironically, named Freeman, Walter Jackson Freeman II (1895-1972), to be exact.
Some famous victims of lobotomy were Rosemary Kennedy, the sister of US President John F. Kennedy, and Evita Perón, wife of Argentine president Juan Peron.
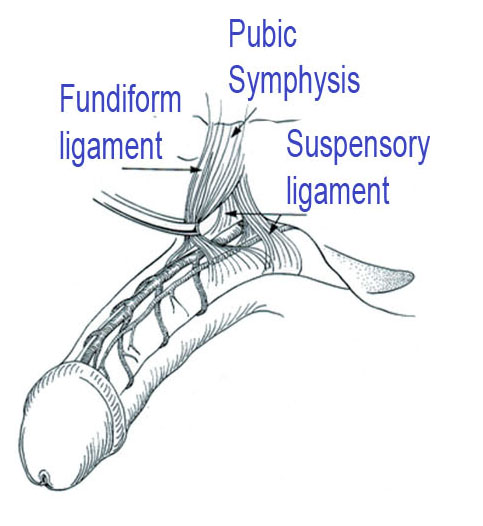
In the mood for surgery on another precious organ? Augmentation phalloplasty?
Mind you: elective surgery is the preferred business model of physicians who drive Ferrari and plan for a yacht.
Various surgical penis enlargement procedures are on the market.
Karimi, Faith (2018), New York man wins $343.8 million Powerball jackpot by playing same numbers for 25 yearsCNN, https://edition.cnn.com/2018/11/15/us/robert-bailey-powerball-winner-trnd/index.html
Landau, Elizabeth (2010), Awake during surgery: 'I'm in hell' CNN Health
http://edition.cnn.com/2010/HEALTH/05/17/general.anesthesia/index.html
Lenzer, Jeanne (2012), UNNECESSARY CARE Is profit driven healthcare to blame? Overtreatment, https://www.bmj.com/bmj/section-pdf/187652?path=/bmj/345/7877/Feature.full.pdf
Kremer, William (2016), Paolo Macchiarini: A surgeon’s downfall BBC News
https://www.bbc.com/news/magazine-37311038
Madani, Doha (2018), New York winner of $343M Powerball jackpot wants to avoid the pitfalls of instant wealth NBC News https://www.nbcnews.com/news/us-news/new-york-winner-343m-powerball-jackpot-wants-avoid-pitfalls-instant-n936306
Michaleas, Spyros N.; Laios, Konstantinos; Tsoucalas, Gregory; Androutsos, Georges (2021) Theophrastus Bombastus Von Hohenheim (Paracelsus) (1493–1541): The eminent physician and pioneer of toxicology, Toxicology Reports
Volume 8, Pages 411-414, https://doi.org/10.1016/j.toxrep.2021.02.012
Nix, Elizabeth (2023), 7 Things You May Not Know About Howard Hughes, History, https://www.history.com/news/7-things-you-may-not-know-about-howard-hughes
Szabo, Liza (2018) Surgery Near End of Life Is Common, Costly, Kaiser Health News
https://www.scientificamerican.com/article/surgery-near-end-of-life-is-common-costly/
Tan, Siang Yong MD JD; Yip, Angela MS2 (2014),
António Egas Moniz (1874–1955): Lobotomy pioneer and Nobel laureate, Singapore Medical Journal, Vol 55(4), Pages 175–176, https://doi.org/10.11622%2Fsmedj.2014048
Top 10 Largest Insurance Companies in the World by Asset Size in 2020, Insurance Industry Factsheet BizVibe
https://blog.bizvibe.com/blog/largest-insurance-companies
Wikipedia, Paolo Macchiarini, https://en.wikipedia.org/wiki/Paolo_Macchiarini
By tongkatali.org
tongkataliorg3@gmail.com
Updated May 13, 2023






References:
